Researchers at the University of Oxford compared the aptitudes of the Victoria virus (from the 1st wave) and the B.1.1.7 UK variant when confronted with large numbers of antibodies, by carrying out in vitro neutralization testing. In their own stock of the most effective antibodies that they have previously characterized (see the precedent article by the same authors) 19 target the RBD (where binding with ACE2 occurs) and one targets the N-terminal domain (NTD), where there is no interaction with ACE2.
The study also included certain antibodies that are referenced and used in emergency treatment, as well as antibodies that emerged from 2 clinical trials (Astrazeneca, Regeneron) and from blood samples taken from convalescing patients (some of whom were infected with B.1.1.7) or vaccinated patients (Astrazeneca, Pfizer). Overall, these neutralizing antibodies were very effective against the Victoria strain and less so against the B.1.1.7 variant, but the results were not constant. The reduction in effectiveness was very marked in certain antibodies but not all.
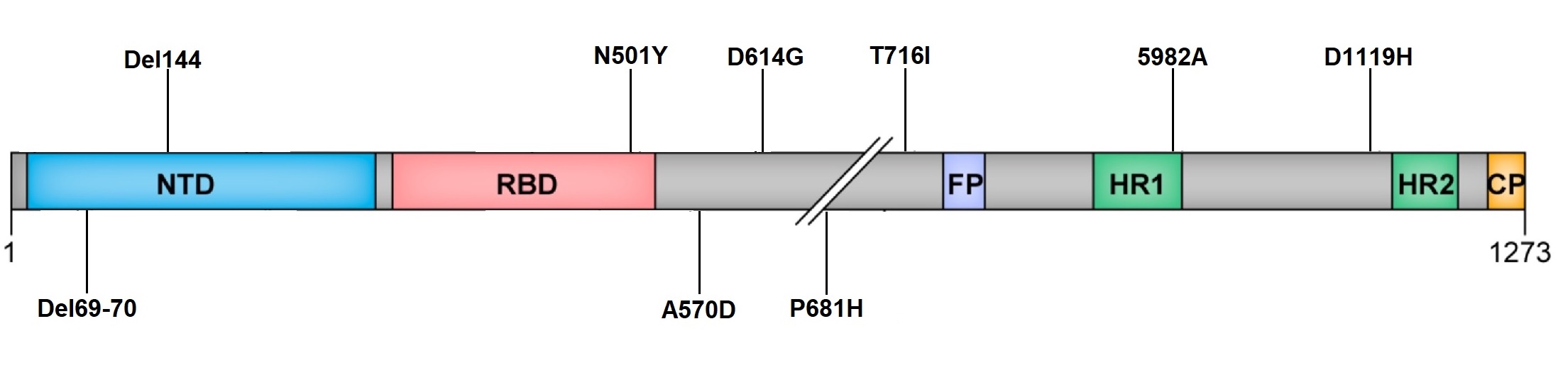
Using the BLI technique (Biolayer Interferometry), researchers showed that the N501Y mutation alone (a mutation common to the UK, South African and Brazilian variants) increases the affinity for ACE2 7-fold. This increase goes along with a reduction in neutralizing power of the antibodies. Anti-NTD antibodies, which do not target the RBD, reduce this link by a factor of 5,7 though we do not know why. Mathematical modelling and structural analysis (crystallography) show that the antibodies lose their neutralizing power by entering into competition with ACE2 for fixation points on the RBD. It is principally the N501Y mutation that enfeebles the antibodies’ binding. Certain antibodies that are referenced and currently used in treatment do not neutralize the B.1.1.7, because of altered interaction with the 501 amino acid. The influence of the 69-70 and 144 deletions is less significant.
In conclusion, protection given by antibodies directed against a strain from the 1st wave decreases, but remains strong against the UK variant. There is, therefore, no substantial evasion of the vaccine, which suggests that current vaccines will remain effective against this strain. In addition, several other mechanisms are involved in providing protection: the T response, the antibody Fc function (see letter News-COVID-19.info February 22-28, 2021) and complement activation. It has not yet been ascertained if the 3 variants (UK, South African and Brazilian) lead to more severe symptoms or if they enable in vivo evasion. Certain vaccines are currently being tweaked to deal with these variants. Janssen and Novavax have recently said that they have candidate vaccines against the UK variant. It is not known whether the protection resulting from one of the 3 variants is effective against the others or against strains deriving from the 1st wave.