During the COVID-19 pandemic there has been much talk about monoclonal antibodies (mAb). The technique, however, is not new. Monoclonal antibodies have revolutionised the treatment of many illnesses such as cancer, auto-immune and inflammatory illnesses, and infectious diseases, and they can limit transplant rejection. Early serotherapy dates back to 1890, since patients could acquire passive immunity against tetanus or diphtheria through the transfusion of blood from humans or from surviving animals (polyclonal antibodies recognizing multiple targets).
MAbs recognise a single target and act either by blocking the target’s functions or by recruiting other immune factors via their Fc domain (effector functions). The neutralising antibodies are able to block the viral entry by binding either to the virus or to the receptor of the target cell. In 1998, palivizumab was the first neutralising mAb to provide therapeutic benefits in the treatment of pneumonia caused by the Respiratory Syncytial Virus (RSV). However, this approach later demonstrated limited effectiveness in the treatment of respiratory illness. Recently, several mAbs showed promise for the treatment of Ebola, influenza A or HIV, using prophylactic (preventative) or therapeutic (treatment) approaches. With any given virus, the mAbs must target as many strains as possible and impede the emergence of escape variants. The scientific literature does not indicate clear evidence of synergy when several non-competitive mAbs are used in combination.
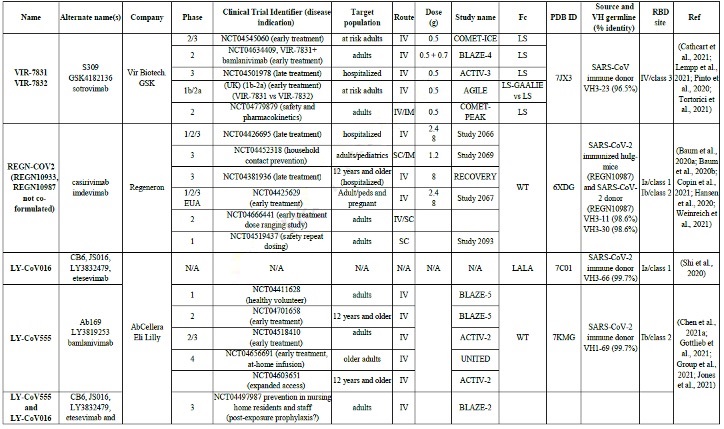
Recently, worldwide efforts to combat COVID-19 has enabled the development of medicines and vaccines with a level of effectiveness never before seen. RECOVERY was the most important clinical trial to evaluate the effectiveness of treatment by anti-SARS-CoV-2 antibodies (amongst others) but plasma transfers from convalescing patients were stopped in January 2021 due to a lack of effectiveness. The main problem was the low level of neutralising antibodies contained in this plasma. Amongst the 13 mAbs that are today approved for the treatment of infectious diseases, 6 are used in the urgent treatment of COVID-19 (including bamlanivimab, REGN-COV2, etesevimab and regdanvimab). Numerous other mAbs are currently in development to help curb acute infections.
Where do they come from? These mAbs are taken from humans immunised against SARS-CoV-2 or SARS-CoV (VIR-7831, ADG2), or from humanised (REGN10933, ABBV-47D11) or wild (ABBV-2B04) mice.
But more to the point, how do they work? Whether under development or already authorised, they are all neutralising and targeted against the Receptor Binding Domain (RBD) of the spike, so as to block binding with the ACE2 receptor or other possible co-receptors. Class 1 mAbs recognise the RBM (Receptor Binding Motif) only under the “open” form of the spike (REGN10933, LY-CoV016, AZD8895, Brii-196, ADG2, CT-P59, ABBV-2B04) whereas the class 2 mAbs recognise it under both its forms (LY-CoV555, AZD1061, BGB-DXP593). The VIR-7831 recognises the glycan (complex sugar) in position N343. In certain cases, these mAbs can render the spike inactive by causing a structural change to its fusion form. Some may block it by keeping it in its closed conformation (C144). Although other mAbs target alternative domains to the RBM (cryptic sites, N-terminal domain), none is being developed. The effector functions of the mAbs are currently being evaluated, because some data suggests these functions may worsen the infection (Antibody-Dependent Enhancement, ADE). As a precaution, 5 mAbs, currently in development, have been modified to abolish or modify these functions (including VIR-7831, VIR-7832, ADG2).
How effective are they? When the first mAbs were authorised, the current variants had not yet formed. Since the SARS-CoV-2 rate of mutation is relatively weak, immune escape was underestimated. It was also thought that anti-RBM mAbs would limit this phenomenom since the RBM site is highly conserved (it mutates little since it is essential to the virus).
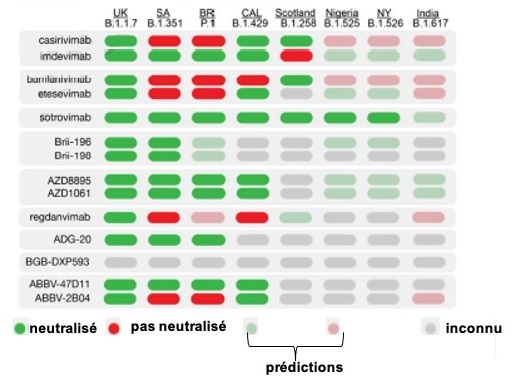
However, recent studies have shown that they are relatively permeable to mutations. Pushed by immune pressures, SARS-CoV-2 initially mutated to D416G. When this strain became dominant, it opened the way to several others, which represent 90% of current sequencing: the UK variant (B.1.1.7, new WHO nomenclature: alpha a); the South African variant (B.1.351, new WHO nomenclature: beta, b); the Indian variants (B.1.617.1, new WHO nomenclature: kappa, k; B.1.617.2, new WHO nomenclature: delta, d); the Nigerian variant (B.1.525, new WHO nomenclature: eta, h); the New York variant (B.1.526, new WHO nomenclature: iota, i); the Brazilian variants (P.1, new WHO nomenclature: gamma, g; P.2, new WHO nomenclature: zeta, z); the Californian variants (B.1.427/B.1.429, new WHO nomenclature: epsilon, e); the Scottish variant (B.1.258); and the Liverpool variant (A.23.1). These mutations are often linked to increased transmissibility, and some are able to escape several mAbs, which have for this reason been removed from clinical trials. Bamlanivimab, the REGN-COV2 cocktails (casirivimab+imdevimab) and ABBV-2B04+ABBV-47D11 are sensitive to the E484K and K417N/T mutations found in the B.1.351, B.1.525, B.1.526, A.23.1 and P.1 variants. On the other hand, the mAbs that are not affected by these mutations are being studied closely (VIR-7831, COV2-2196).