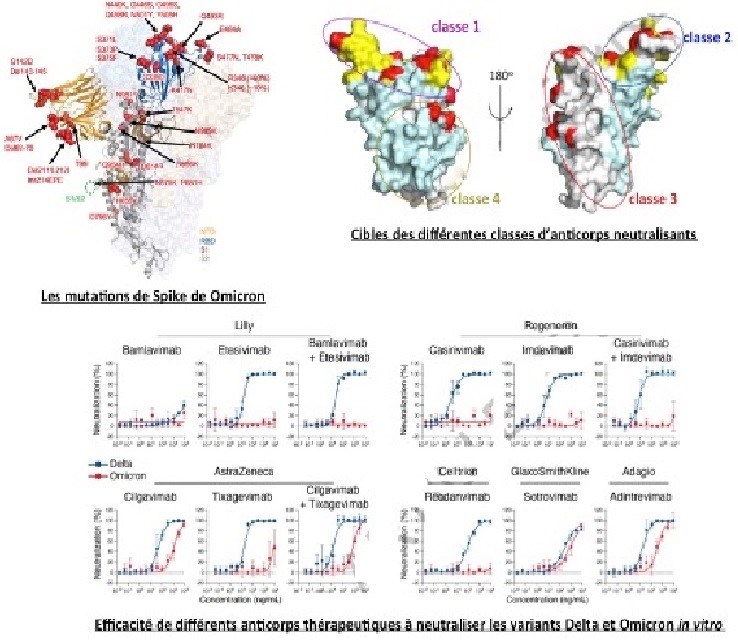
Another study, by French researchers (at the Institut Pasteur de Paris) and Belgian researchers (at the University Hospital of Leuven), reached similar conclusions. They isolated the Omicron variant in a non-vaccinated traveller who arrived in Belgium from Egypt, then made a structural model from its protein sequence. As in the previous study, they confirmed that Omicron mutations alter the binding of 4 classes of neutralising antibodies. Amongst 9 therapeutic antibodies, 6 were ineffective against Omicron (including Bamlanivimab, which also fails to neutralise Delta), while the others had 20 times less effectiveness since they bonded less well with the spike (Cilgavimab, Andintrevimab). Only Sotrovimab neutralised Omicron as well as it neutralised Delta, but with 3 times less effectiveness than against D416G.
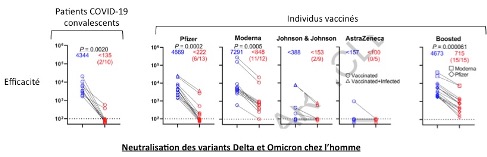
The antibodies of 54 vaccinated individuals (16 Pfizer-BioNTech, 18 Astrazeneca, and 20 having received 3 doses of Pfizer) were then analysed to evaluate their capacity to neutralise Omicron, Delta, or the ancestral strain D416G. The samples were taken 5 months after the 2nd injection and 1 month after the 3rd, and levels of neutralising antibodies were low since they had decreased over time. The results showed effective antiviral activity against D416G, weaker activity against Delta, and none at all against Omicron. The 3rd dose re-established a strong capability of neutralisation against the 3 strains, and increased levels of antibodies by up to 49 times. Neutralisation of Omicron was 18 times weaker than against D416G and 6 times weaker than against Delta. With a cohort of 40 convalescent COVID-19 patients, the results were similar. Between 6 and 12 months after the appearance of symptoms, levels of antibodies capable of neutralising D416G or Delta were relatively stable and about 2 times higher than in vaccinated individuals, but they were incapable of neutralising Omicron in the case of 2/3 of patients. A booster dose of Pfizer-BioNTech increased levels of antibodies targeting D416G 137-fold, and restored the capacity to neutralise Omicron in all patients. Here its efficacy was reduced 53 times as compared to D416G and 23 times as compared to Delta.
Omicron has therefore opened a new chapter in the COVID-19 pandemic, and these studies show how it is able to spread so efficiently within an immunised population. Vaccinated individuals or those already infected remain at risk from Omicron, and antibody therapy is no longer effective. The previous variants had developed resistance against class 1 and class 2 antibodies in particular, and those targeting the NTD. Omicron, for its part, is resistant to all classes of neutralising antibodies. If this variant acquires 2 or 3 additional mutations in strategic areas of the spike, it will become completely resistant. It is therefore imperative that vaccines and antibody therapies are reformulated. But this time, the most conserved regions of the virus must be targeted so that the vaccinal strategy remains effective long-term. In the meantime, booster doses need to be massively deployed, though we do not know how long this will be a useful tactic.