The purpose of virus detection is to identify and isolate COVID-19 patients so as to limit transmission and control the outbreak. But positive cases have been largely under-estimated since many of them are asymptomatic or cause only slight symptoms, and so are not counted. At the beginning of the epidemic, because nothing like this had ever been encountered, France’s logistical capabilities for testing were insufficient and concentrated only on serious cases. But in order to bring the first lockdown to an end (on the 11th of May 2020), it was decided that all potential cases should be systematically tested.
In order to evaluate the efficiency of this policy and to ascertain its limitations, French researchers at INSERM, Sorbonne-Université used computers to model the evolution of detection rates in 12 French regions between the 11th of May and the 28th of June, the 7 weeks after the end of the first lockdown. The model was based on virological data (PCR) and centred on the SI-DEP (a secure platform where COVID-19 test lab results are systematically recorded), on polls (7500 people responded on COVIDnet.fr) and on demographic and behavioural studies. It took a number of factors into account: the various degrees of severity, lockdown, reduction in numbers of contacts after hospitalisation or self-isolation, relaxation of social distancing measures over time, the partial resumption of normal activity, and increased risks for the elderly. The model’s projections were also compared to independent serological (detection of antibodies) and virological surveys.
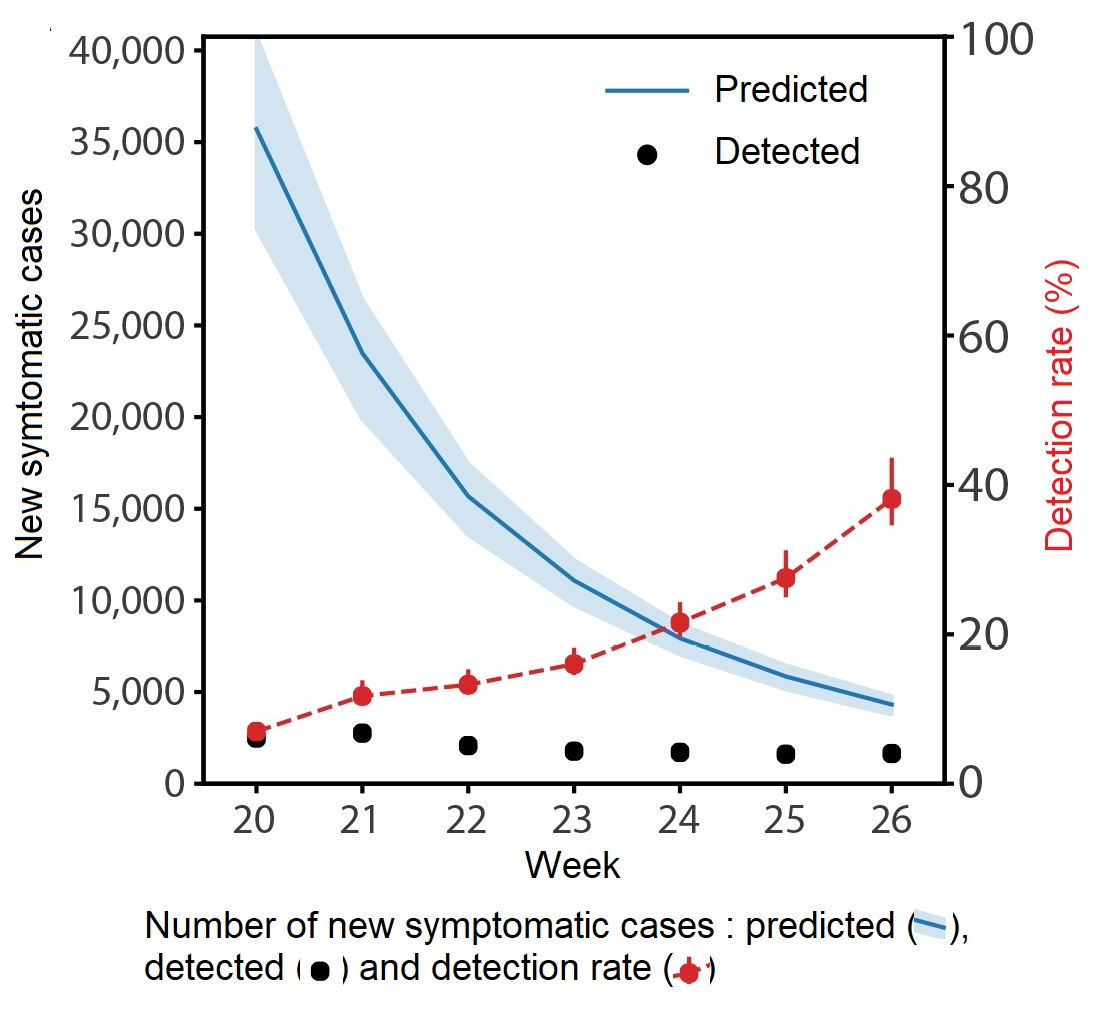
We now believe that the real number of cases greatly exceeded cases confirmed at the time. An average of 9 symptomatic cases out of every 10 may not have been identified. Over this period, the expected average detection rate evolved from 7 to 38% as a result of a reduction in infections (end of the first wave) and a progressive improvement in systems of detection (prescriptions were no longer required, PCR “drive” tests developed mobile applications were implemented and delays between symptom onset and test were reduced).