It has now been established that following SARS-CoV-2 infection, we efficiently generate antibodies against the virus. Some of these, the neutralizing antibodies, have the potential to block the binding of the virus to a target cell, but it has not yet been clearly established if they can give protection against new infection by the same virus. However, reported cases of reinfection are rare, which gives us some cause for optimism.
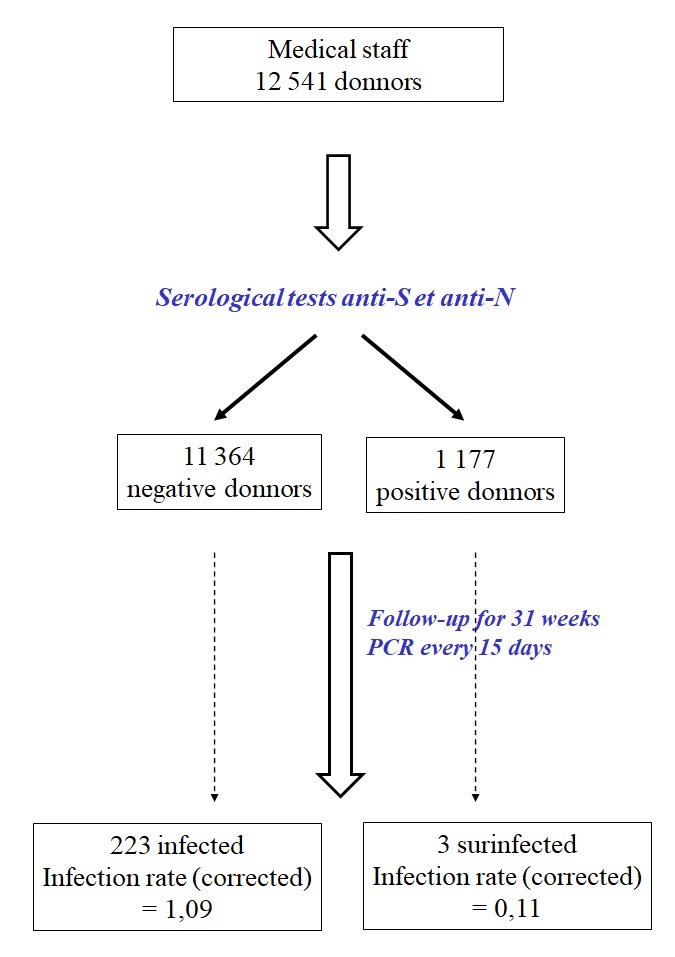
In order to look at this question in more depth, researchers at Oxford (United Kingdom) studied medical staff from 4 hospitals affiliated to the University over a period of 31 weeks. The researchers looked at the presence of antibodies in the blood working against the spike protein (S, the target of neutralising antibodies) or against the nucleoprotein (N, an internal protein not subject to neutralisation) by ELISA tests, which are serologic tests specifically for the detection of antibodies against COVID. After having determined if they were positive or negative, they examined, every 2 weeks, using PCR, whether they had contracted the virus during this period.
At the beginning of the study, 11 364 participants, that is, more than 90%, tested negative. 1 177 participants were positive. Amongst the latter, 68% had had COVID-19 symptoms, and 37% had tested positive with PCR.
At the end of the study, 223 negative participants had been infected: 100 were asymptomatic and 123 showed symptoms. Only 3 positive participants had been reinfected (all asymptomatic), and only one had previously tested positive with PCR. These 3 participants had discordant levels of anti-S (2 out of 3) and anti-N antibodies, while only one had developed both antibodies. This reveals that the use of ELISA to detect antibodies as primary infection markers is unreliable.
Since the risk of infection was inconsistent (notably between the two first waves) the rate of infection was modelled according to the Poisson regression statistical model and adjusted according to age, sex and time: this rate was found to be 1,09 for negative cases (of which 0,6 were symptomatic) and 0,11 for positive cases.