The Johnson & Johnson vaccine is an adenovirus vectored vaccine expressing the spike protein of the Wuhan ancestral strain. It has 85% efficacy against severe forms of the disease and is administered in a single dose. It is helpful for countries with difficulties accessing vaccines. However, while we know that a supplementary dose of an mRNA vaccine increases the efficacy of the immune response against variants of concern (VoC), this question has not been resolved for the Johnson & Johnson vaccine.
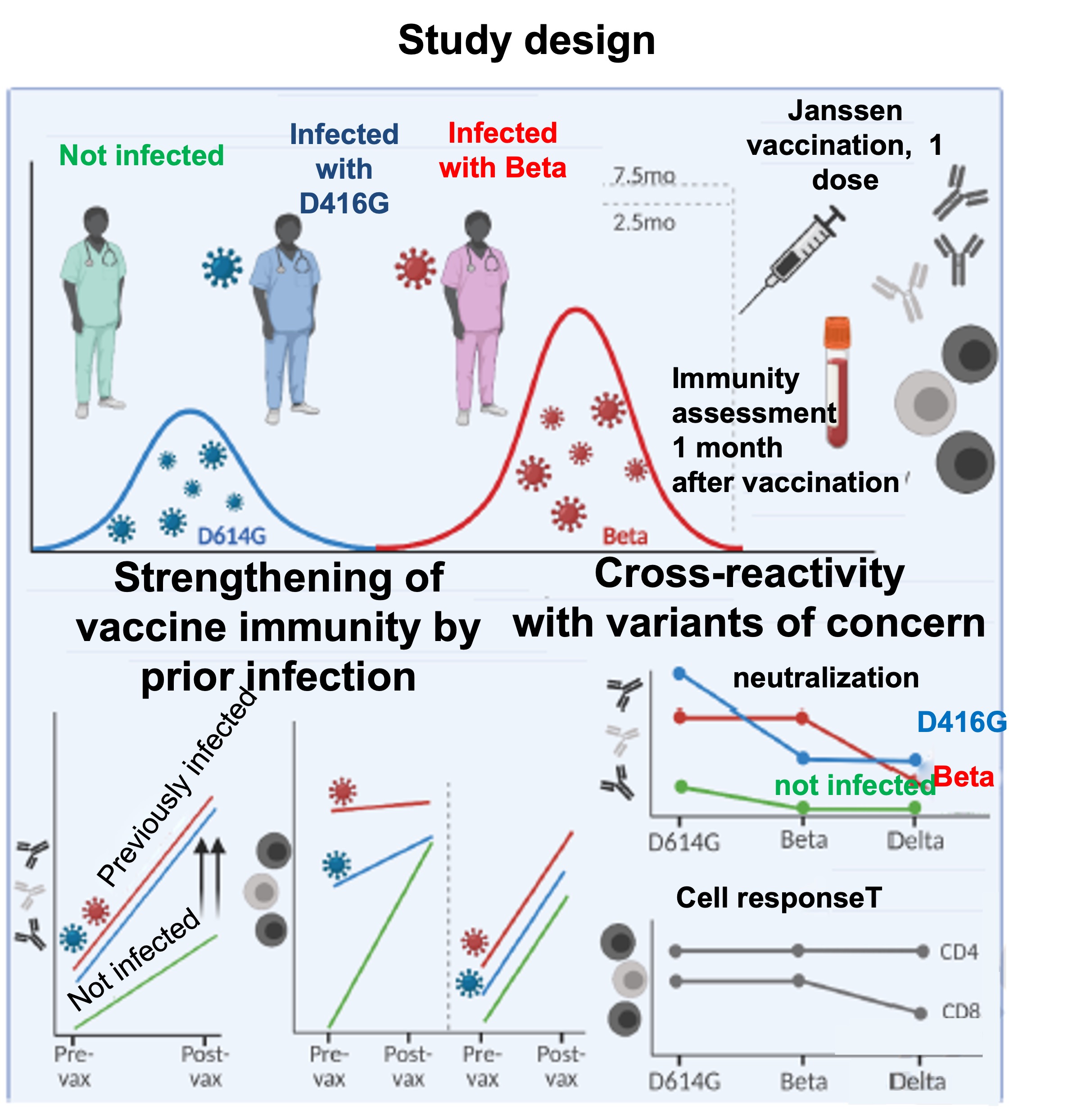
In order to provide answers, South African researchers (at the University of Cape Town) carried out a study. It should be noted that South Africa experienced a first wave of infections dominated by the D416G variant in summer 2020, followed by a second wave dominated by the Beta variant in November 2020. The scientific approach of the researchers involved the observation of healthcare workers vaccinated with the Johnson & Johnson vaccine, and divided into 3 groups:
- 20 workers who had never been infected
- 20 workers with prior infection by the D416G ancestral variant
- 20 workers with prior infection by the Beta (South African) variant
Serological samples were taken from the participants.
What were the main observations?
One month after vaccination, the 3 groups showed equivalent levels of anti-spike antibodies (neutralising and non-neutralising) that recognised both the D416G and Beta variants.
One month later, the 2 infected groups showed levels that were 3 times higher. The level of neutralising antibodies was relatively small in the non-infected group, while this figure increased 12- or 13-fold in the 2 infected groups. In the non-infected group, the antibodies of only 15% of participants were capable of neutralising Beta, with 22% able to neutralise Delta. Cross-neutralisation was much higher after infection. However, the group infected with D416G neutralised Beta and Delta less effectively than D416G, while the group infected with Beta was able to neutralise D416G and Beta in a similar way, but efficacy was reduced 6-fold against Delta.
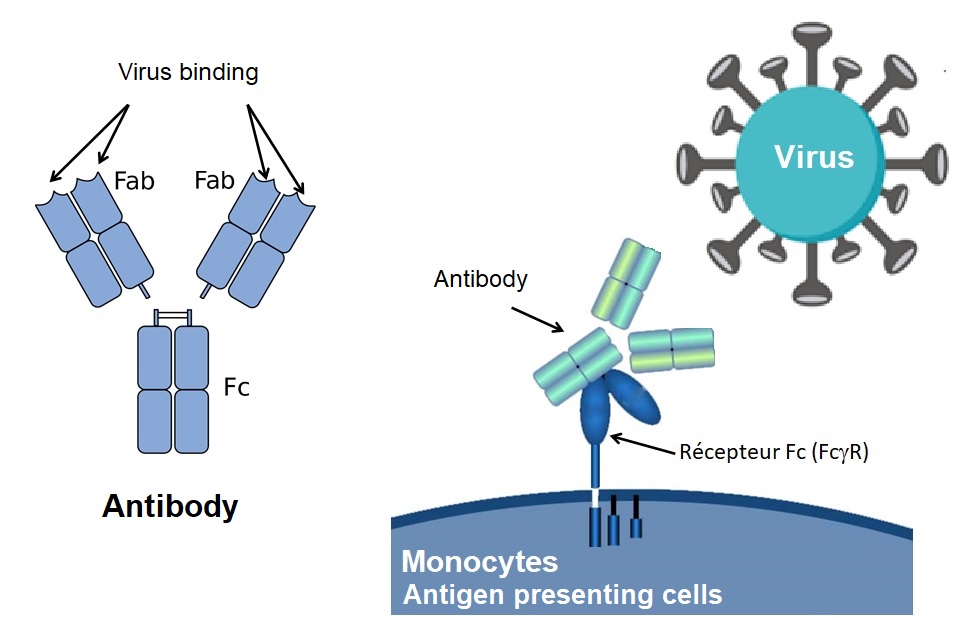
The infected groups showed a better Fc effector response to the same degree against D416G, Beta and Delta (immune cells recognise antibodies by their non-pathogen-specific ‘tail’). Unlike the neutralising response, the Fc response showed effective cross-reactivity against the Beta and Delta VoC, irrespective of whether this was induced by a single vaccination or not.