The most recent large-scale epidemics (flu, Zika, Ebola, COVID-19) have underlined the importance of developing models to predict the spread of illness. In particular, they help in the implementation of appropriate public health measures. The first such model, dating from 1927, focussed principally on population density. But in order to be effective, these models need to take into account behavioural and social elements, determining factors in the evolution of emerging diseases. For example, individuals will tend to follow public health measures according to their own perception of danger, their beliefs and traditions, their trust in government, their own health, and their social or geographic situation.
Modelling these factors is a complex undertaking and they can be interpreted in different ways. There are, therefore, several competing blueprints which can be distinguished by their presuppositions and their advantages and disadvantages. They can be summarised as follows:
- “Economic” epidemiology tries to forecast behaviour according to the illness’ prevalence. If there is high risk of infection, individuals will adopt preventative measures (isolation, social distancing, vaccination or the purchase of condoms in the case of STDs), all of which will have economic and social consequences, taken into account in these models. The researchers will therefore assume that human behaviour is always rational when confronted by illness, which is far from being the case (emotional factors, fear, etc.).
- Epidemiology may also be modelled according to social network dynamics. This strategy analyses the transmission of the disease by contacts, but also by behavioural changes brought on by the transmission of information (vaccination campaigns, public health alerts). For example, if we are informed that a friend is ill, we can choose not to see him/her for a while.
- Modelling based on “associated contagions” concentrates on the influence of emotions. Concretely, fear (of the illness or of vaccination) is transmitted in the same way as a virus and influences the behaviour of individuals, thereby modifying the epidemic’s own dynamic. But other emotions, such as trust in science or in politicians, are not integrated.
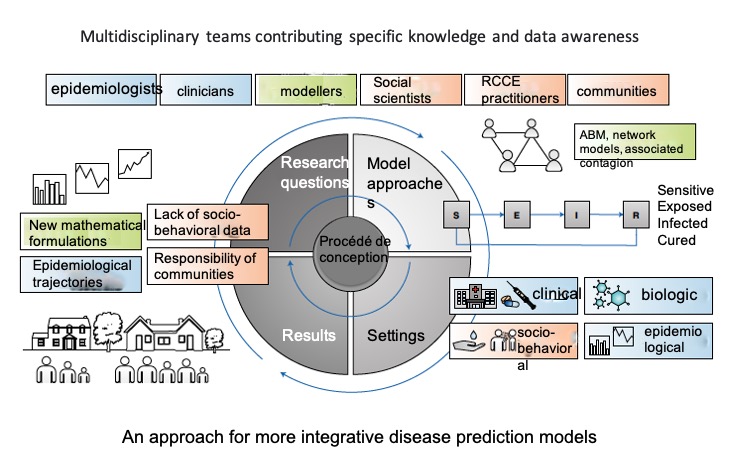
- Agent-based modelling (ABM), probably the most fully developed system, analyses the transmission of the virus through representative individuals (active or passive agents) who are associated in homogenous groups according to diverse criteria (socioeconomical, clinical and environmental). Each individual (and his/her characteristics) is explicitly represented. The system has been developed over the last 20 years and these models can account for the behavioural dynamics of a population with heterogeneous communities.
All these models are imperfect since they do not integrate all factors able to influence an epidemic, such as access to health care or the mobility of populations. For this reason, investment in social sciences and in risk communication has been reinforced in recent years (Risk Communication and Community Engagement, RCCE). In the context of an epidemic, social sciences help the understanding of structural, environmental and behavioural factors influencing propagation dynamics. Closely linked, RCCE practices are based on working with communities, civil societies, governments, opinion groups and leaders to better identify emergencies. In coordination with local or international (UNICEF) groups, they reinforce the mobilisation and the organisation of the community. Risk communication must provide information in real time so as to rapidly determine sanitary strategies, but also needs to manage the kind of “fake news” that can have damaging consequences.
It is clear that forecasting human behaviour is a complex task that mathematical models tend to simplify. But to perfect them, we must find standards (measures, indicators) applicable to all countries, in order to standardize practices. In addition, many of the disciplines involved collaborate very little between each other. It is therefore necessary to create a dedicated transdisciplinary community of practitioners and to develop a common framework to understand and interpret this social and behavioural data, which is scarce, difficult to gather (especially in a period of crisis) and should be more accessible.
It is for these reasons that the vocation of the RCCE Collective Service, a platform co-ordinated by the World Health Organisation, UNICEF and the International Red Cross, is to optimise the collection of data and to share information systematically, internationally, and in a standardised way. This involves a great deal of work with specialists in this area and the attendant financial consequences.
With these forecasting models, mathematicians, social science professionals and practitioners of RCCE have as a shared objective to reduce mortality and the “foreseeable” socioeconomic costs linked to the spread of a disease. The precision of these models is thus important to be able to guide political strategies and to successfully meet the challenges of emerging diseases.