As the SARS-CoV-2 virus continues to spread and preventative vaccines are rolled out, strategies for treating COVID-19 remain necessary. The virus replication cycle is made up of numerous stages, each one a potential area for therapeutic intervention. This includes blocking the virus penetration, interesting since the medicine does not need to enter the targeted cell.
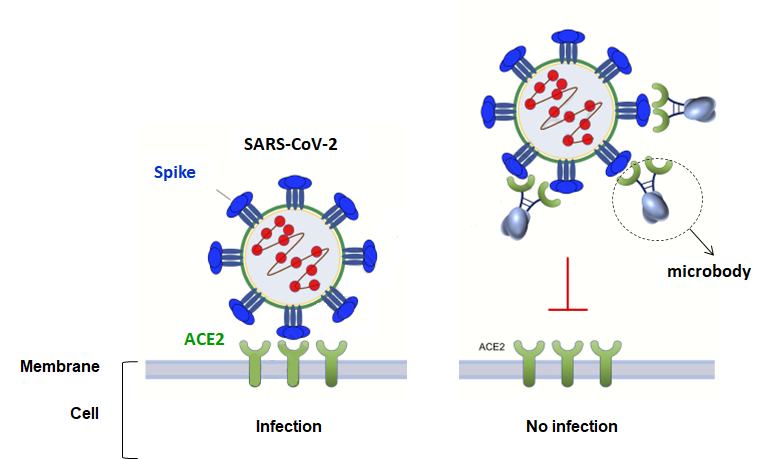
To go into detail, the SARS-CoV-2 spike protein binds with its ACE2 (Angiotensin-Converting Enzyme 2) receptor, exposed on the external surface of the cell. The normal physiological role of ACE2 is to help regulate arterial pressure and cardiac function. After the spike-ACE2 interaction, the viral envelope and the cellular plasma membrane merge to enable the entry of the virus.
In order to block this entry, therapies based on administering neutralizing antibodies are being developed. However, their effect can be mitigated by spike mutations allowing certain variants to escape. The use of soluble ACE2 receptors, which fix themselves to the spike, means that this problem can be overcome, since the virus needs to attach itself to its receptor. In this strategy, already explored in VIH-1 research, the part of the receptor that allows it to anchor itself to the cell is cut off, and this action may be enhanced by a fragment of antibody (Fc region) to optimize and stabilize its effect.
The first trials on SARS-CoV-1 (which spread through thirty or so countries in 2002-2003, infecting about 8 000 people and causing about 800 deaths), then on SARS-CoV-2, at the origin of the current pandemic, showed that soluble receptors are effective in blocking the entry of the virus in vitro, but problems with stability occurred in vivo in mice. In humans (phase 1 and phase 2 clinical trials on SARS-CoV-1) the antiviral effects had only partial success for the same reasons.
Other difficulties exist too. Firstly, these soluble receptors can attach themselves to immune cells, favouring infection rather than prevention. And in mice, the fact that ACE2 is still active in excessive quantities in the organism can bring about a fall in arterial pressure.
This is why researchers in New York constructed a “microbody”, where the ACE2 was disactivated then coupled to domain 3 of the Fc region of an antibody. Compared to other approaches, the microbody, much smaller, shows a greater affinity for the virus and does not target immune cells .