The clinical evolution of COVID-19 differs greatly from one patient to another: there may be few or no symptoms, only moderate illness and complete recovery, severe illness with a developing acute respiratory distress (SARS), or multiple organ failure and eventual death. Several factors influence this development: age, genetic or immune system predispositions, obesity, diabetes, or cardiovascular illness. Although the divergence of symptoms between patients is still poorly understood, it is related in particular to a lack of coordination between B and T immune responses or high levels of pro-inflammatory cytokines. In responding to SARS-CoV-2, numerous complex immune system mechanisms are triggered and their development involves diverse cells that communicate between themselves.
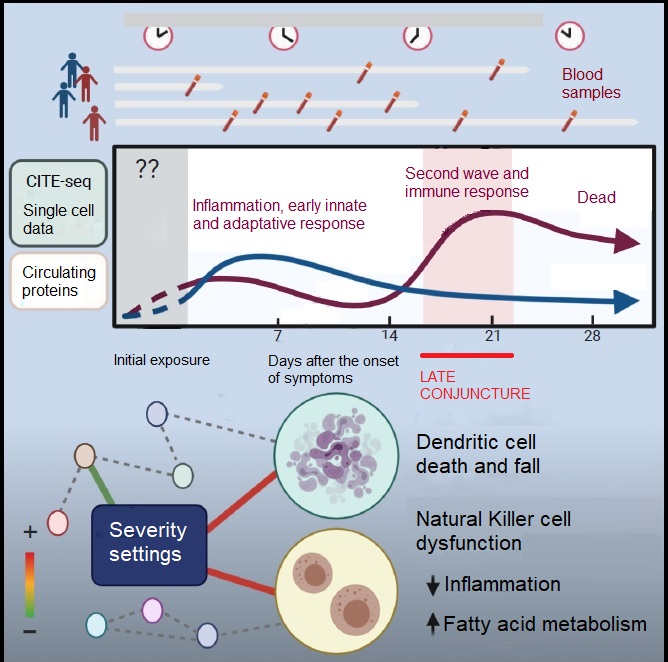
To better understand what defines the severity of the disease as seen in blood activity, researchers at the NIH (Bethesda, USA) carried out a multiparametric and longitudinal follow-up (up to + 40 days according to each case) of 33 hospitalized COVID-19 patients. Using blood mononucleated cells (PBMC), this simultaneous single-cell-scale analysis (CITE-seq) evaluated gene expression levels of 188 surface proteins, but also global genes (mRNA transcriptome) and the sequence of antibodies and receptors. It also took into account levels of circulating proteins (including cytokines) over time and the characterization of different blood cell populations. This data was processed using computer modelling, then compared to results from other independent cohorts, in order to find correlations.
This study revealed indicators in the blood in severely ill patients. It was seen that there exists a network of specific “signatures” (over or under-expression of particular genes) linked to the severity of the illness.
It seems that the timing of the analysis is crucial to be able to evaluate responses to the infection. The first samples (T0) were taken an average of 11 days after the appearance of symptoms, at the time of hospitalization. Several major events can be listed:
- a fall in the interferon type 1 response (IFN, linked with innate immunity and inflammation) in the PBMC was observed from T0, more sudden in critical patients and more progressive in less severe cases.
- a fall in levels of dendritic blood cells (involved in adaptive response triggering and producing IFN) was also observed. This fall could be due to the apoptosis of these cells (programmed death) for unknown reasons.
- the NK CD56dimCD16hi cells (Natural Killers, lymphocytes belonging to the innate immune response which destroy infected cells) seem to stop functioning: the expression of genes involved in inflammation (INFgamma, NF-kB, mTORC1) falls, but that of genes involved in the metabolism of fatty acids (amongst others) increases, and this correlates with levels of circulating IL-15. The reasons are unknown, but this is probably a sign of malfunctioning. These cells lose their ability to destroy infected cells, which is their principal role.
- in severely ill patients, inflammation which began at low levels became elevated between days 17-23, signifying typical hyper-inflammation. The researchers suggest that this late second wave may be triggered by bacterial superinfections, because they detected specific markers (LBP, lipocalin-2) at this precise time. The damage observed in the tissues and organs of these patients enables a transfer of commensal bacteria from one organ to another. This phenomenom has already been observed during severe flu infections.