Infection by SARS-CoV-2 leads in 15% of cases to severe illness associated with respiratory distress syndrome and increased morbidity and mortality. The difficulties of taking samples from patients, often limited to broncho-alveolar fluids, hinders understanding of the consequences of infection at lung tissue level.
Researchers at the University of Columbia instigated a programme of rapid autopsies (under the direction of the Institutional Review Board) to remove and freeze the pulmonary tissues of COVID-19 patients in the ten hours following their deaths, so avoiding any deterioration. They analysed transcription profiles (transcriptome) by single-cell RNA sequencing (snRNA-seq). This work was carried out on a cohort of 19 people with an average age of 72 as well as on a control-cohort (non COVID-19) of 7 patients aged about 70, representing a total of 116 314 cells. The cells were identified and classified according to several criteria, such as markers expressed in the membrane (over or under-expression of specific genes) or their granularity (which reflects the internal complexity of the cell). In total, 9 cellular types were identified: epithelial and endothelial cells, myeloids, fibroblasts, T and B lymphocytes, neurons, mastocytes and antigen-presenting cells (including dendritic cells).
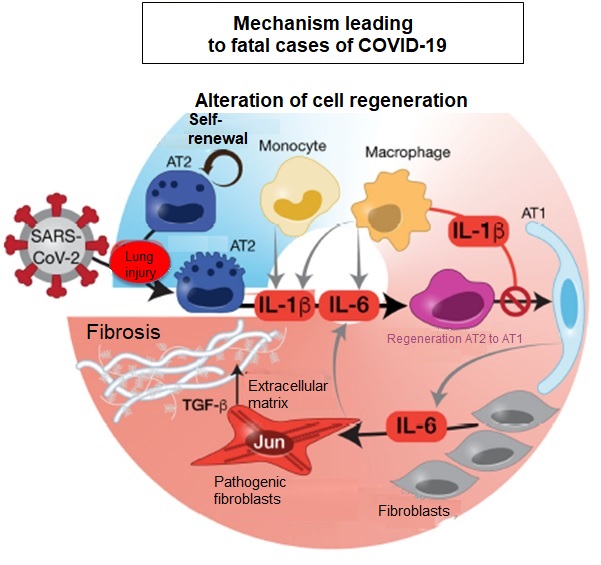
In COVID-19 patients overall, an increase in the number of myeloid cells was observed, in particular monocytes and macrophages that were aberrantly overactivated (over-expression of CTSB/D/Z, PSAP). This suggests that these cells are a major source of inflammatory deregulation in the lungs. The analysis of blood cells showed that antibody response was relatively well preserved (enrichment of the IGHV1-18/IGLV3-20 genetic combination producing neutralising antibodies). In COVID-19 patients, the number of alveolar cells (AT1 et AT2) was seen to be reduced. AT2 cells, which act as progenitor cells to regenerate the AT1 cells, can no longer make this transition (decrease in ETV5, CAV1).
By using a supplementary cohort of 23 patients and proteomic analyses, the researchers showed that the epithelial cells produce more IL-6 and the macrophages produce more IL-1β, two pro-inflammatory cytokines overexpressed in COVID-19 patients, compared to healthy patients or patients suffering from other pulmonary infections. Tuft cells (overexpression of ChAT, Pou2f3), involved in the inflammation of respiratory passages but whose role is little understood, were 3 times more present in the upper respiratory passages. The number of fibroblasts was also higher, in particular pathological fibroblasts (overexpression of CTHRC1, JunB/D).