Cellular ageing is a multifactorial process of molecular changes leading to the progressive degradation of biological functions. It is a major risk factor for many illnesses (cancer, heart attacks, pneumonia…) that occur in the context of COVID-19. These changes can be detected in the genome, in intracellular signalling, in organelles and in the cellular phenotype. The populations of Western societies are becoming proportionately older than ever before. For example, in the United States, the number of elderly people will be greater than numbers of children in 2034. In the light of this perspective, it has become essential to better understand the biological mechanisms of ageing, which in turn will help us to understand aspects of the COVID-19 crisis.
The lungs play a major role in the general health of individuals, and the progressive change in their functioning due to age (from 35 years old) is directly linked to the risk of illnesses, whether respiratory or not. The lungs make up a unique interface between our internal tissues and the external environment (and its aggressors). The lungs are the organ of the human body with the greatest surface area and are made up of 40 different types of cells organised into strata. Age increases the risk of chronic obstructive inflammation, interstitial fibrosis (the over-75s have a 50 times greater risk than 18-34 years old) and lung cancer. With an ageing population, the rate of incidence of cancers is increasing. Cancer of the lungs causes the most deaths (25%), despite there being 5 drug treatments approved by the FDA (Food and Drug Administration). Respiratory infections are a major cause of death in elderly people, in particular pneumococcus and influenza (30 times more risk of death).
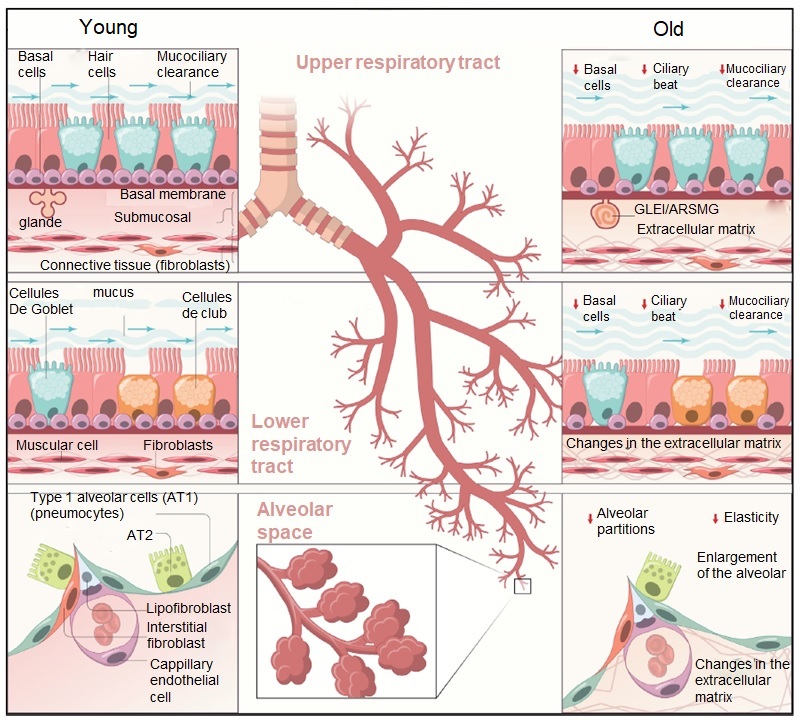
In general the ageing process shows itself by changes in morphology and physiology. Progressive decline can be seen in the alveolar surface, in elasticity, in self-cleaning (mucociliary clearance) and in defence reflexes (mechanical cleaning)
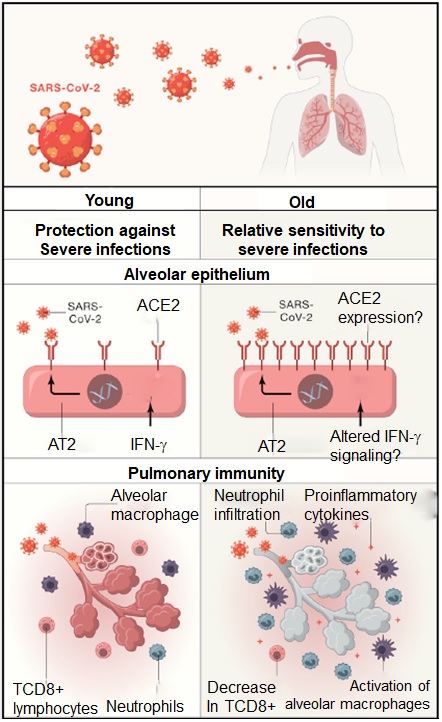
It appears that each of these cellular activities undergoes specific alterations that have consequences in the case of infection by SARS-CoV-2. More particularly, the respiratory epithelium makes up the first line of defence between the exterior environment and our internal tissues. Ageing brings about a decline in epigenetic regulation (gene expression profile changes), telomere shortening, and changes in the functioning and production of mitochondria (the powerhouses of our cells).
In this alveolar epithelium, which in the main consists of type 1 pneumocytes (AT1), the AT2 are the progenitor stem cells that enable the repair and regeneration of the respiratory system, and also produce the pulmonary surfactant (a surface-active complex necessary for respiratory function). These cells lose the ability to renew and differentiate themselves, and to metabolize the lipids that make up the surfactant or recognize the self (MHC). The interstitial medium (space between the cells) is essential to the functioning, elasticity and cohesion of the entire pulmonary environment. Its functioning also declines with age since the fibroblasts become senescent (risk of fibrosis) and certain metabolisms (collagen, elastin, laminin, fibronectin) undergo gradual modification, all of which increases rigidity.
The lungs have to be able to cope in the face of the constant stress factors (materials, aerosols, pollutants, radiation, chemical agents, lesions, cigarettes or hypoxia) to which they are exposed. But their resistance mechanisms also change with age. The proteostasis network – the system of mechanisms that regulate the “life” of proteins – becomes less efficient. This is the case with the autophagy process that normally degrades poorly synthesized proteins or internalized external agents. When it fails, proteolytic stress and fibrosis are more likely. This is particularly significant for the AT2 cells that synthesise and secrete many components to produce surfactant.
The degradation of dysfunctional mitochondria (mitophagy), a typical feature of pulmonary fibrosis, is also impaired, due to deregulation of the expression of certain genes (PINK1, Parkin). In addition to other consequences, responses to hypoxia (lack of oxygen) are deregulated in the AT2 cells, which contain more than 50% of pulmonary mitochondria and which maintain energy balance in anaerobic conditions (disturbances in the mTOR, AMPK, and HIF2 channels).
Responses to oxydative stress are also altered. The ROS (Reactive Oxygen Species) are metabolic intermediates of oxygen, developed endogenously (mitochondria) or exogenously (cigarette smoke), which accumulate with age. Their levels must be precisely regulated (this is the role of antioxidants) since their accumulation in cells causes mutations in DNA and the oxidation of neighbouring molecules. These molecules thus lose their functions and need to be degraded, but they accumulate since the process of autophagy is less efficient. Elevated levels of ROS are linked with lung cancers, with fibrosis, and with pulmonary hypertension, problems which are particularly accentuated by cigarette smoke. This cellular stress slows mucociliary clearance and thus makes infections and accumulation of debris more likely. As with other tissues, senescence (the stopping of cellular division) plays an important role in this overall weakening of the lungs, notably at the level of interstitial cell remodelling.