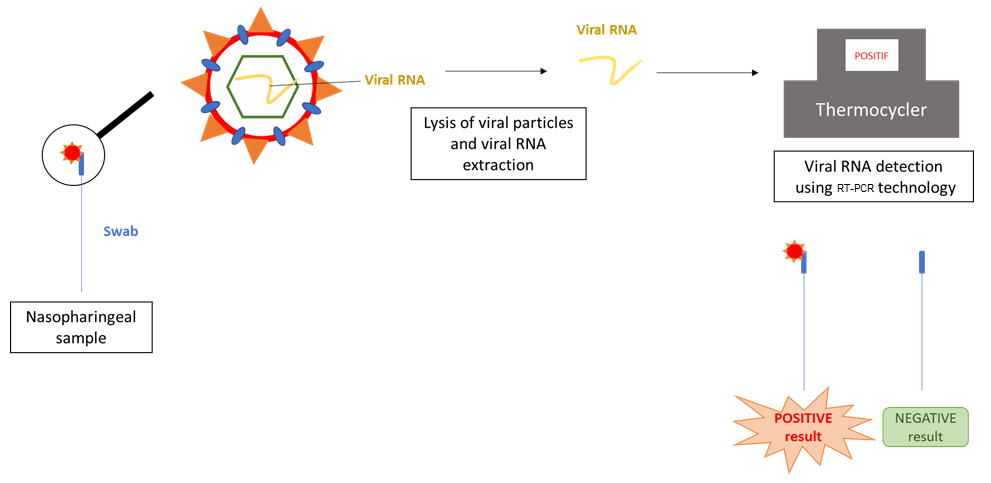
The RT-PCR COVID-19 diagnostic test allows to detect the presence of virus in a patient at the time of sampling only. It is based on viral RNA detection and realized from nasopharyngeal swabbing. From this sample, a viral particles lysis and a viral RNA extraction were realized and allow to detect this RNA using a machine called thermocycler. This test should be acheived in the laboratory.
In asymptomatic patients, levels of viral RNA and of the detected virus are comparable. Immunocompromised patients are more likely to develop severe cases of respiratory infection, such as SARS-CoV-2 or flu. This condition affects about 3 million people in the United States, for diverse reasons: pathologies (AIDS), anti-rejection treatments after transplants, chemotherapy treatment, anti-inflammatory treatments (corticoids)…
A recent clinical study described the particular case of a 71 year old immunocompromised patient suffering from chronic leukemia and hypogammaglobulinemia (low levels of antibodies). She was admitted as an emergency due to problems linked to her leukemia and was found to test positive by RT-PCR for SARS-CoV-2. She remained positive for 105 days, and infectious viral particles were present in the nasopharynx for up to 70 days after the first test. Her case was therefore of extremely long persistence.
Since this patient had a low natural production of antibodies, she received two anti-SARS-CoV-2 antibody treatments intravenously, from convalescing donors. This treatment had mixed results, but nevertheless the patient remained asymptomatic during the whole period of infection.
In the majority of COVID-19 cases, very little variation has been seen in individual patients: the virus which infects the patient undergoes little mutation when it replicates, probably due to the pressure of selection in the immune system. In this patient, the viral populations (detected by high-throughput sequencing technology) were very changeable, principally concerning the spike protein. The virus’ capacity for replication and infection were unaltered, as shown by infection tests in vitro and detection of subgenomic RNA (which confirms viral activity). The patient was therefore highly contagious.
Although these results need to be confirmed by a larger sample of patients, we can come to several conclusions arising from this study :
1) Immunocompromised patients tend to be RT-PCR-positive and contagious for much longer than other patients, without necessarily showing symptoms. Their potential to contaminate is high and they may also spread mutated forms of the virus.
2) The recommended strategy of using the RT-PCR test (detection of genomic RNA) in cases where there are established symptoms is not suitable for evaluating these patients’ levels of contagiousness. Subgenomic detection of RNA should be used as a complement.
3) Therapies using passive immunity are usually reserved for patients with severe or critical cases of COVID-19, but would seem to have limited effectiveness because antibodies administered intravenously struggle to reach the nasopharynx.