SARS-CoV-2 has infected 106 million people and killed 2.3 million. Several candidate vaccines have been developed by different companies (Novavax, Janssen, Moderna, Pfizer-BioNTech, Oxford-AstraZeneca), based on various technologies (RNA, adenovirus vectors…). All these vaccines have been developed using sequences of the surface spike (S) viral protein from the strain in Wuhan that was at the origin of the epidemic. Now the virus has mutated. We have to ask ourselves whether those vaccines already developed will remain effective.
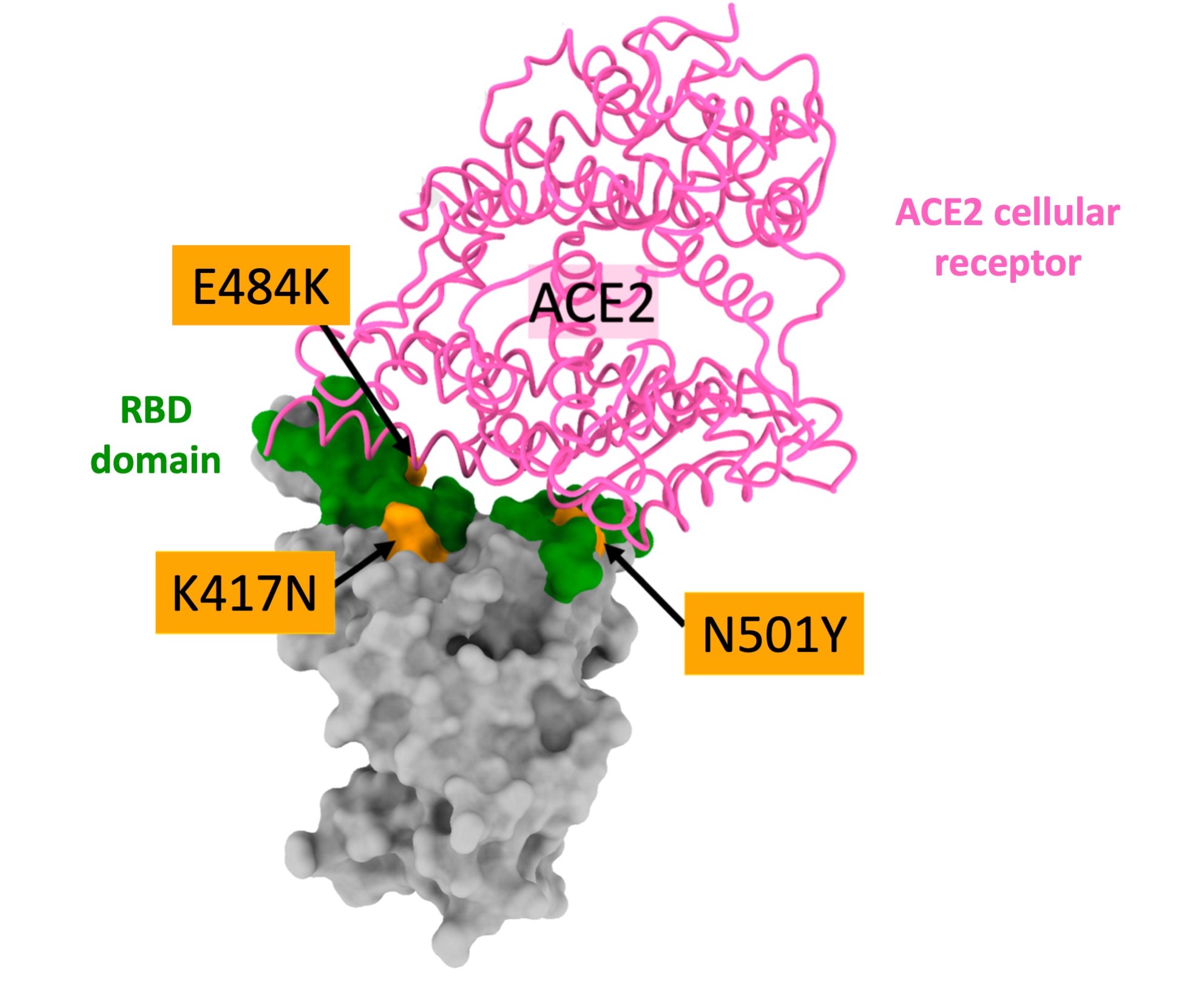
In the course of recent weeks, a number of variants have appeared in different parts of the world. The 1st to be identified was the UK variant in October 2020. Others were then reported, notably the South African variant in October and the Brazilian variant in December. These new viral strains each have 9 to 12 mutations or deletions, mainly in the S protein, but with a common point: certain mutations are found in the RBD domain. The RBD (“Receptor Binding Domain”) is the region of the S protein that binds to the ACE2 cellular receptor, enabling the viral particle to enter the cell. This region is also the target for numerous neutralizing antibodies. Protection against infection, whether acquired naturally or through vaccination, depends on the blockage of this interaction between the RBD and the ACE2 cellular receptor.
The 3 variants have developed mutations within the RBD: N501Y in the UK variant, K417N, E484K and N501Y in the South African, and K417T, E484K and N501Y in the Brazilian. These mutations seem to give the 3 variants greater transmissibility, confirmed by the UK strain. This selective advantage has enabled them to quickly become majority strains in the areas where they have appeared.